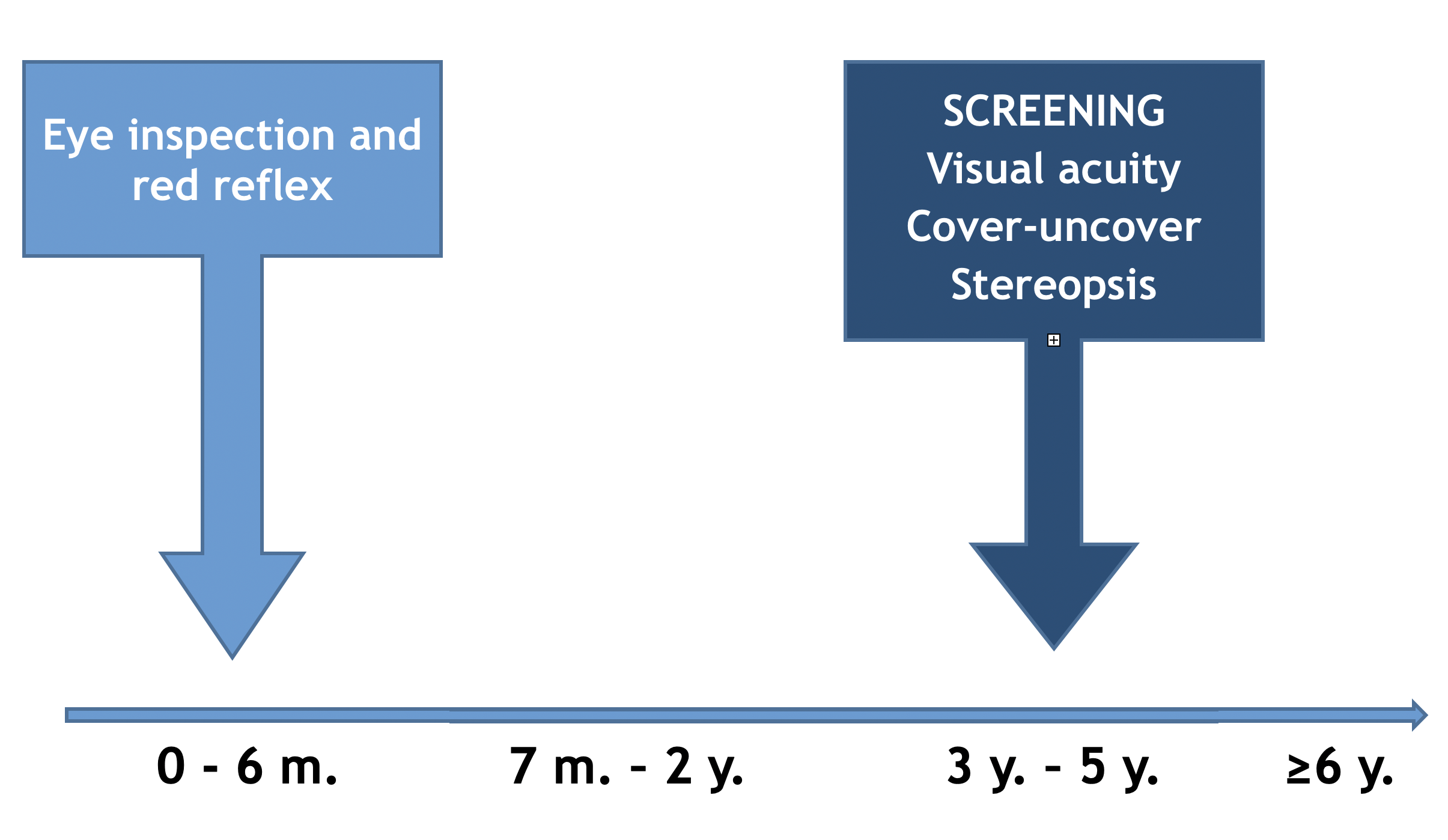
Visual disorders screening in children is relevant for the early detection of those impairments that can cause problems in visual development, in school performance, or sometimes, as in retinoblastoma, maybe life threatening. In newborns and infants, the screening aims to the early detection of eye problems such as congenital cataract or retinoblastoma. In preschoolers, its objective is amblyopia and the detection of its risk factors, such as strabismus or refraction errors. In the school age, screening consists in low visual acuity detection due to refraction errors.
Evidence on the benefits of newborn and infant visual screening is scarce and it is not possible to produce a recommendation based on the balance of benefits and risks. Nevertheless, the impact on health of potentially severe conditions such as congenital cataract or retinoblastoma and the proven effectiveness of early interventions to improve the prognosis of these conditions, justify the inclusion of ocular inspection and red reflex test as an essential component of newborn and infant physical exam.
There is moderate certainty that amblyopia and amblyogenic factors’ screening in children 3 to 5 years old produce a moderate net benefit. Although there is no direct evidence on the global benefits of screening, in terms of indirect evidence there are proofs that are reasonably valid for the identification of children with visual problems. Moreover, the treatment of amblyopia or unilateral refractive errors is associated to an improvement of visual acuity, what suggests that with early detection programs more cases would be detected, and better visual results would be obtained than in the absence of screening.
Evidence on school age visual screening is insufficient to stablish a balance on benefits and harms. Its effectivity is unknown. The measure of visual acuity offers a good sensitivity and specificity for the detection of myopia but is not very precise in the detection of hypermetropia and astigmatism. The treatment of refractive errors in asymptomatic children has not proven to produce better results than the treatment when symptoms appear.
PrevInfad recommendations
-
PrevInfad recommends ocular inspection and red reflex test in each well-child visit on the first six months of life, considering that, although the quality of evidence is poor, the expected balance of the intervention is probably positive.
Grade of recommendation: given that the red reflex test does not meet the necessary conditions to be considered a screening test, it is not possible to establish a grade of recommendation for the newborns and infants' visual disorders screening.
|
-
PrevInfad recommends visual disorders screening (amblyopia, strabismus and refraction errors) at the age of 3 to 5 years old.
Grade of recommendation B.
|
|
|
Visual screening in childhood
Grade of recommendation
Detection of amblyopia and its risk factors in 3 to 5 years olds: B
Detection of low visual acuity in school age children: I
Criteria for referral to the ophthalmologist in low risk children
| 0 to 5 months |
- Ocular disorders such as ptosis, corneal lesions, leukocoria or nystagmus
- Absent or asymmetrical red reflex
- Fix strabismus |
| 6 to 35 months |
- Difficulties for monocular object fixing and following
- Absent or asymmetrical red reflex
- Any alignment problem |
| 3 years* |
- Visual acuity less than 0.4 logMAR (2/5 Snellen, 0.4 decimal) monocular
Should identify correctly most of optotypes in the 0.5 decimal line |
| 4 years* |
- Visual acuity less than 0.3 logMAR (1/2 Snellen, 0.5 decimal) monocular
Should identify correctly most of optotypes in the 0.5 decimal line |
| 5 years* |
- Visual acuity less than 0.2 logMAR (2/3.2 Snellen, 0.63 decimal) monocular**
Should identify correctly most of optotypes in the 0.63 decimal line |
*It is also a referral reason any alignment defect or the absence of stereoscopic vision.
**Or the 0.66 (2/3) line if the optotype does not have 0.63 line.
How to cite this article: Jaime García Aguado. Visual screening in childhood. Recommendation. In Recomendaciones PrevInfad/PAPPS [online]. Updated July 2016. [consulted MM-DD-YYYY]. Available in http://previnfad.aepap.org/recomendacion-en/vision-enrec











